
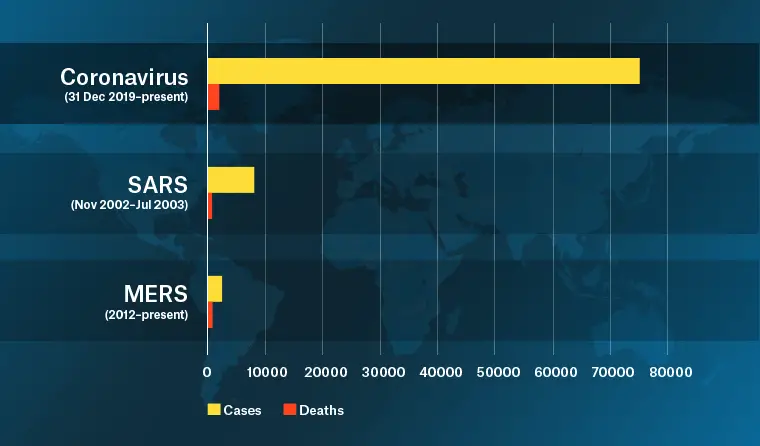
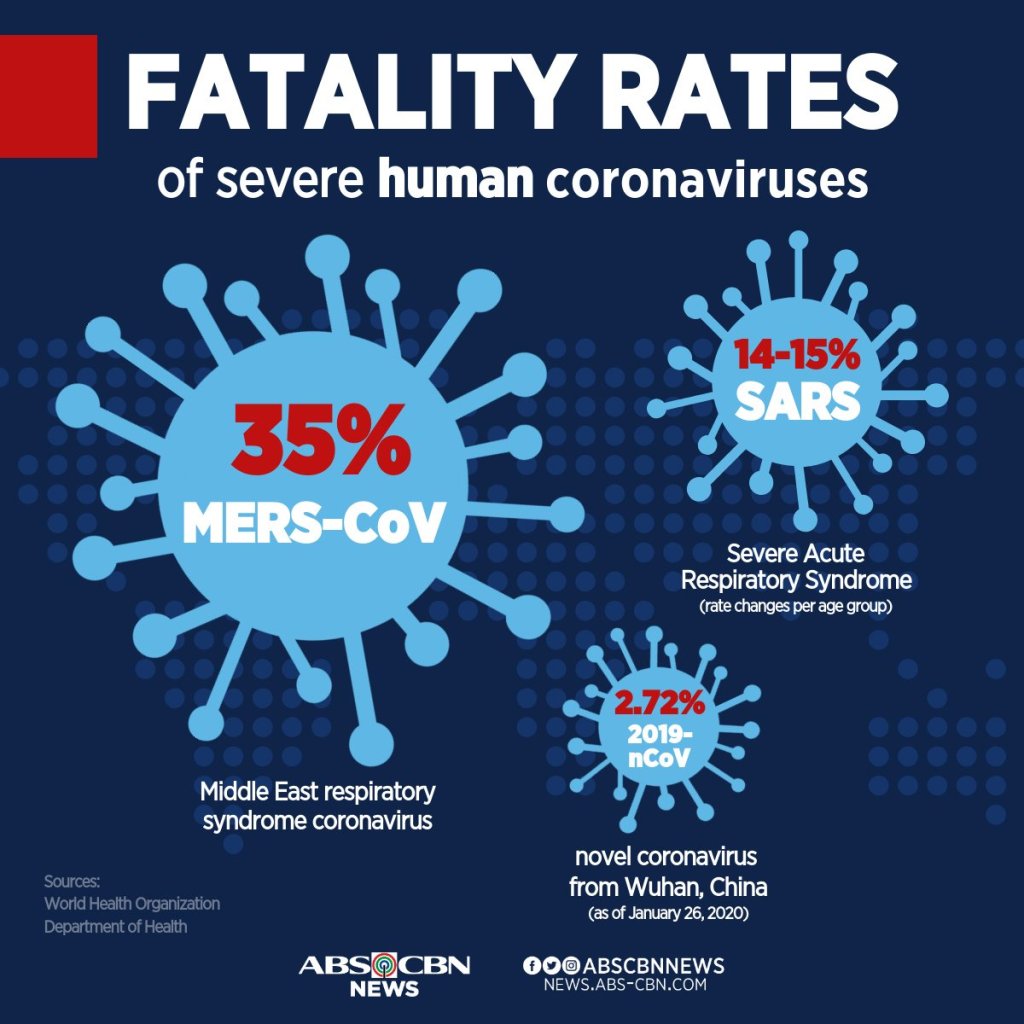
There’s no doubt as to the seriousness of SARS-CoV-2 (the causal agent of COVID-19 disease), indeed this was highlighted by the World Health Organization giving this epidemic the status of a Public Health Emergency of International Concern (PHEIC) on January 30 – you can read the minutes of the meeting where the declaration was made > (https://www.who.int/news-room/detail/30-01-2020-statement-on-the-second-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-outbreak-of-novel-coronavirus-(2019-ncov). However, hysteria aside, we need to put it into perspective. As of today, there are 76 819 reported cases and 2 250 deaths – certainly serious by any measure. This of course may be under reported and needs to be taken as a guide only. Interestingly, this current global figure is similar to what the actual number of cases in Wuhan alone was predicted to be as at January 25, from the work of Wu et al. (2020), researchers from the The University of Hong Kong. Therefore, from the “official” figures, the crude calculation of case fatality rate (CFR) of this disease, which is currently at 2.5% needs to be taken very much as a guide only and treated with a great deal of caution. While the total number of reported cases is clearly substantially greater than SARS in 2002-2003 and MERS in 2012 (Figure 1), it offers some (and I stress, some) guidance. Whatever the situation turns out to be, the CFR rate is on the low side when compared with SARS and MERS (Figure 2), with younger healthy people rarely succumbing to the disease, meaning those that are in their senior years or immunocomprised in some way represent those that typically die from the COVID-19 disease.
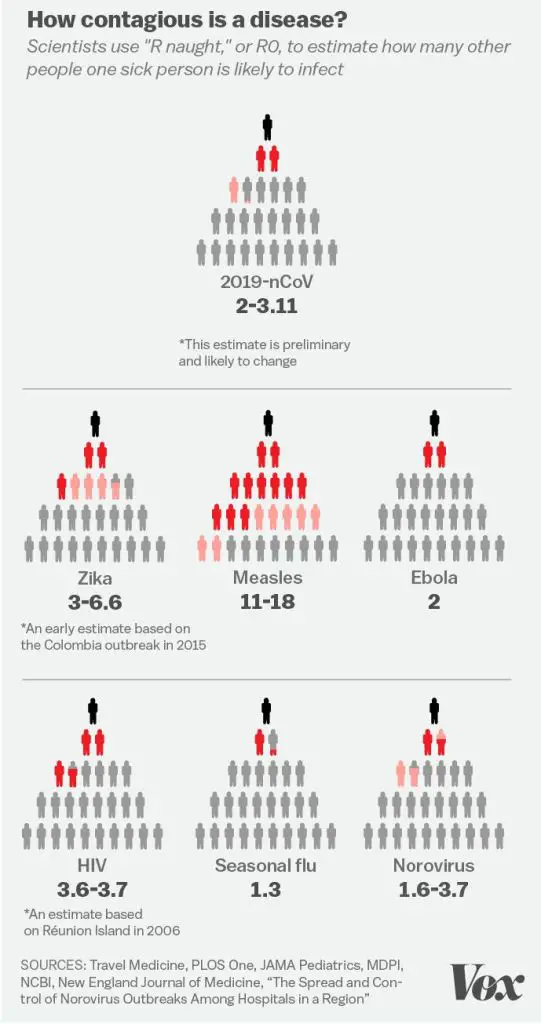
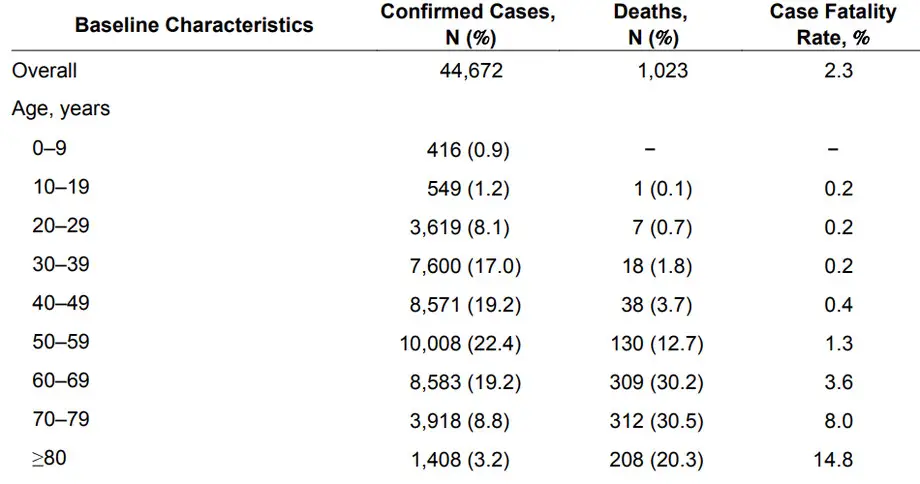
An important epidemiological concept to consider is the Basic Reproduction Number, known as “R0”. This number describes how quickly an infectious agent spreads, and is basically related to how many people one infected individual can infect. An excellent article about this concept can be found here > (https://www.vox.com/2020/2/18/21142009/coronavirus-covid19-china-wuhan-deaths-pandemic). The R0 of SARS-CoV-2 is on the low side of the scale (although two to three fold higher than seasonal Influenza) (Figure 3) and if you do acquire the virus, chances of a complete recovery are extremely high. This is especially so if you are in the 10-39 age group, where the CFR is just 0.2% (Figure 4, which shows data from mainland China – data outside of mainland China show even lower CFRs). In practical terms, this means that if you are aged between 10 and 39, and contract the virus, you have a 99.8% chance of making a full recovery. Yet there is great fear amongst people, people taking all kinds of extreme measures to avoid being near people they consider represent ‘typical’ cases of the disease, even in countries like Australia and the US. This irrational behaviour is certainly not justified, especially when one considers other diseases, with high CFRs. Thus, social isolation of particular cultural groups and types of businesses operated by these people are of great concern and impact to (initially) the local economy, but later on, regional and maybe the global economy.
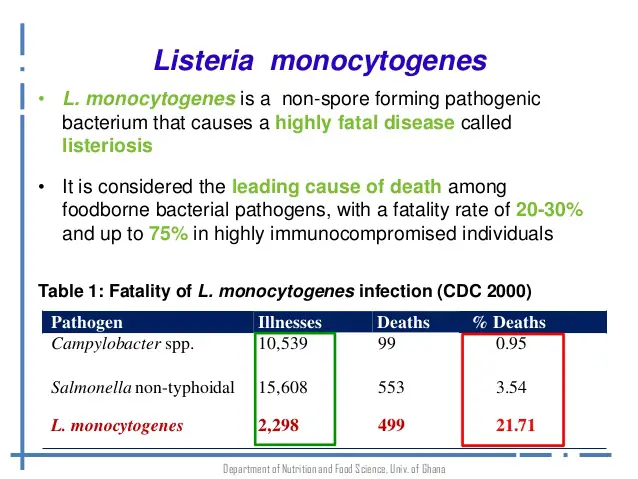
Anyway, as I saying, there are other diseases with much higher CFRs -take listeriosis for example. The CFR for listeriosis tends to hover around 20% overall (Figure 5), and is especially of concern for pregnant women who, if infected in the second or third trimester, are likely to survive, but their fetus will have a mortality rate of around 45%. While this disease is relatively rare, with only 65 cases reported in Australia per year, its high mortality rate warrants extra care regarding exercising preventative measures. Of even greater concern would be infection with Vibrio vulnificus, the CFR of which is typically between 35 and 50% overall (Hlady & Klontz, 1996; Lee et al., 2013), usually due to consumption of raw oysters (Figure 6). Despite this scary statistic, raw oyster consumption (which is the main vehicle of transmission of these bacteria from their natural marine habitat to humans) has remained popular over the years as evidenced by the reported outbreaks (CDC, 1993; CDC, 1996). In fact, people seem to be so keen to consume raw oysters that they stick to belief in various myths they believe can protect them from infection, such as hot sauce and/or lemon juice having a killing effect on the bacteria – this is so not true! In fact, it is laughable, a very humorous myth indeed.
So, am I suggesting or advocating to take a casual stance with regard to SARS-CoV-2? Far from it – what I’m actually saying is put everything into perspective. There are times when one needs to exercise extreme caution, even when it may not seem warranted and times when one can be rather casual. For example, we must think broadly and not only about ourselves. Someone may be young and strong with a top performing immune system, but if their circumstances/actions might put others who are vulnerable, potentially in a bad position health-wise, then we must take more precautions than we consider necessary for ourselves. Take for example, the recent spike of COVID-19 cases in South Korea. Tens of cases are linked to one person, who refused to be tested for SARS-CoV-2, and has infected many people. Even if she was in a low risk demographic (which she wasn’t be the way, being of age 61), she needs to consider that if she is infected, might it be of public health concern? might she infect other people? This is what I mean by putting it all into perspective, considering it on a case-by-case basis and acting accordingly to prevent the spread of the infectious agent and thus doing a favour for your fellow human beings. This is what needs to be paramount in one’s mind amidst a global pandemic, which according to epidemiological projections, won’t peak until April (Wu et al., 2020).
The point to be made here is that there is almost hysteria surrounding infection with SARS-CoV-2, but many people are rather blaise about other infections that are actually severe, with a high death rate – such as Listeria monocytogenes and Vibrio vulnificus discussed above. Please think logically and clearly when making choices and taking actions regarding infectious disease, disease prevention and public health implications – one poor choice can start a global pandemic, that’s all it takes.
References
CDC/Centers for Disease Control and Prevention. (1993). Vibrio vulnificus infections associated with raw oyster consumption–Florida, 1981-1992. MMWR. Morbidity and mortality weekly report, 42(21), 405.
CDC/Centers for Disease Control and Prevention. (1996). Vibrio vulnificus infections associated with eating raw oysters–Los Angeles, 1996. MMWR. Morbidity and mortality weekly report, 45(29), 621.
Hlady, W. G., & Klontz, K. C. (1996). The epidemiology of Vibrio infections in Florida, 1981–1993. Journal of Infectious Diseases, 173(5), 1176-1183.
Lee, S. H., Chung, B. H., & Lee, W. C. (2013). Retrospective analysis of epidemiological aspects of Vibrio vulnificus infections in Korea in 2001–2010. Japanese journal of infectious diseases, 66(4), 331-333.
Wu, J. T., Leung, K., & Leung, G. M. (2020). Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: a modelling study. The Lancet. DOI: https://doi.org/10.1016/S0140-6736(20)30260-9
