

SARS-CoV-2 is a novel Coronavirus that only became known in November or December 2019 in Wuhan, China. It is currently decimating the world population in epic proportions and crippling the global economy. The word “unprecedented” is frequently used to describe events associated with the impacts of this virus, because it is unlike anything that most of us have seen in our lifetimes, and unlikely to ever see again during our lifetime.
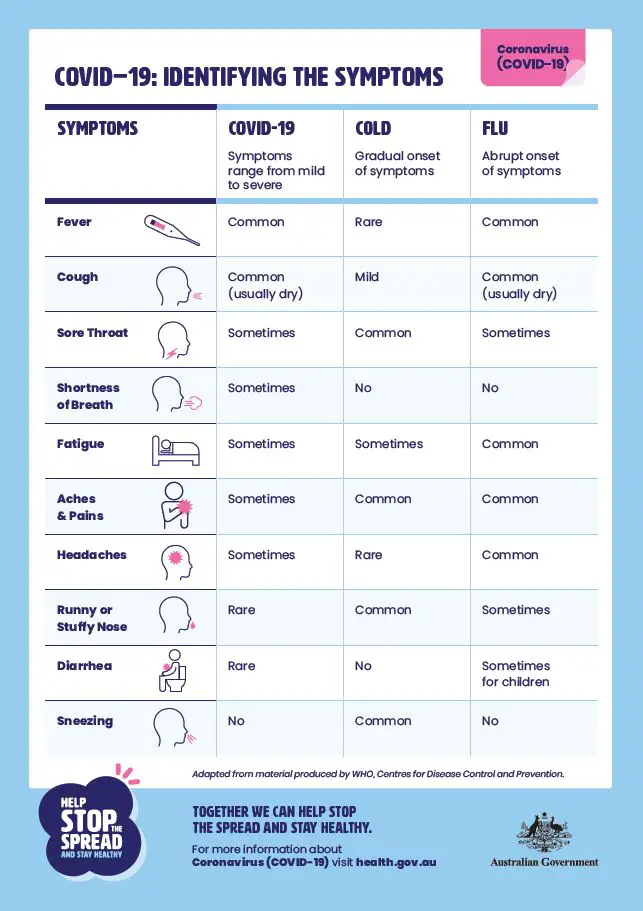
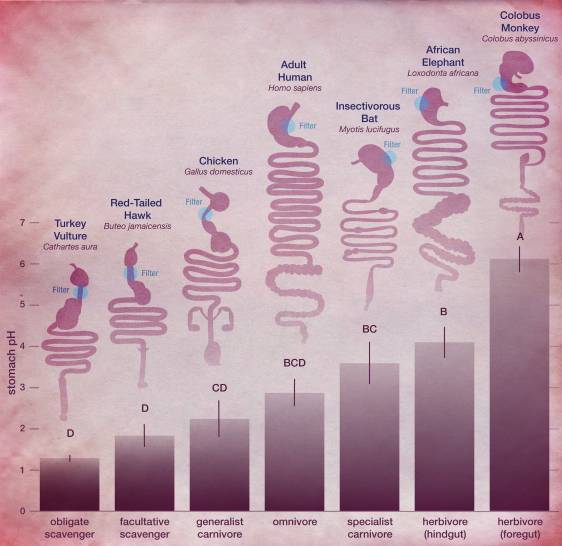
Many of us are very familiar with the symptoms regarded as typical of COVID-19 (Figure 1) – the dry cough and sore throat, fever and headaches, then if it progresses to the lungs, breathing difficulties. As more and more studies are carried out of the many patients, we discover new information about SARS-CoV-2 and COVID-19. For example, a loss of the sense of taste and smell has been seen in some patients as one of the first symptoms. Since early reports of the clinical presentation of this disease, gastrointestinal symptoms have been stated by patients, albeit in much less occurrence compared with the ‘classic’ COVID-19 symptoms stated above. What does this mean? Does the virus effect a gastrointestinal disturbance remotely from the respiratory tract? or in some less frequent situations, has the virus been ingested with food or swallowed with saliva only AND been able to beat the harsh stomach conditions which normally are a formidable barrier to any would-be pathogen seeking to gain entry to the body through the gastrointestinal tract. As a form of non-specific defence, hydrochloric acid in the stomach at a pH of 2.9 (Figure 2) is certainly sufficient to prevent passage of many pathogens. However, not SARS-CoV-2 to an extent – but just we don’t know to what extent. So, does this gastrointestinal involvement add further weight to the speculation of COVID-19 as a foodborne disease? From a scientific perspective, where overwhelming evidence is required to move an idea from speculation to theory to ‘acceptance’, the ‘jury is still out’, so to speak. Let’s look at what the scientific and medical literature tells us and what weight it adds to this theory of COVID-19 being a foodborne disease, in addition to its more traditional aerosol-mediated transmission.
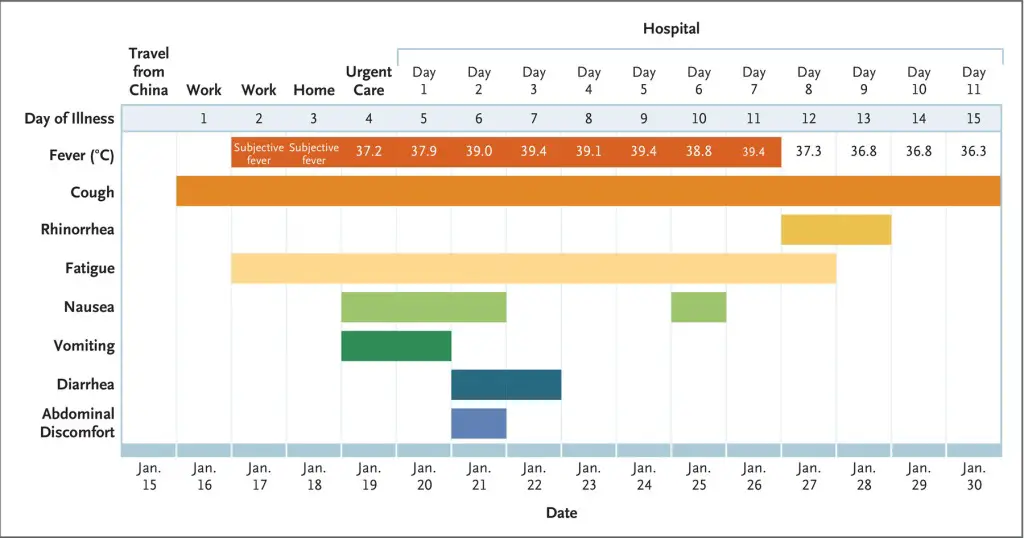
Firstly, Jin et al. (2020) noted that of 651 of the early patients in China between January 17 and February 8, 8.1% reported diarrhoea as their only symptom, while a much smaller proportion reported vomiting (1.7%) or nausea (1.5%) as their only symptom. Guan et al. (2020) studied 1 099 of the early COVID-19 patients in Wuhan and found that 5.8% percent of patients with severe COVID-19 had diarrhoea (with other symptoms) while 6.9% has nausea or vomiting, again, with other symptoms. Yes, these are low numbers compared with the 70.5% with reported coughing, but still, those low numbers outside of the respiratory system seem to suggest something else is happening apart from the classic clinical presentation. Indeed, Gao et al. (2020) states that the connection between the respiratory and gastrointestinal systems is not completely understood. Further interesting results were reported by An et al. (2020) who described nine patients who tested positive for SARS-CoV-2, but only presented with gastrointestinal symptoms. Their gastrointestinal symptoms proceeded their hospital visit by a median of 2.1 days with none of these patients having fever at the onset. Five of those patients went on to develop a fever and/or cough (although not necessarily a dry cough) within two to five days. Interestingly, the remaining four patients developed neither respiratory symptoms nor fever. While a clinical presentation of gastrointestinal symptoms only appears relatively rare, they may not be too uncommon in combination with the more classic COVID-19 symptoms. Figure 1, from Holshue et al. (2020), presents a meaningful diagram of the symptoms experienced by the first positive case reported in the United States – nausea, vomiting, diarrhoea and abdominal discomfort were all experienced by this patient during the course of the illness. Furthermore, Luo et al. (2020) reported an even greater percentage of SARS-CoV-2-positive patients who presented with gastrointestinal symptoms only – a total of 16% from a sample size of 1 141, which were all the patients seen at one hospital in Wuhan between January 1 and February 20. In this study, loss of appetite was the most commonly experienced gastrointestinal symptom.
All these studies, and others, raise the real possibility of a feacal-oral route of transmission, which in at least cases, indicates poor hygiene connected with foodborne transmission. This is supported by the unpublished results quoted by Gu et al. (2020) that two independent laboratories in China isolated infective SARS-CoV-2 viruses (virions) from human stool samples and the report that SARS-CoV-2 has been found in wastewater. Lodder and de Roda Husman (2020) discovered the virus in wastewater at Amsterdam Airport Schiphol, just four days after the first reported case of SARS-CoV-2 infection in the Netherlands.
So, what have we got here – i) a range of gastrointestinal symptoms experienced by a small but certainly not insignificant proportion of SARS-CoV-2 patients, ii) an infectious particle that clearly is not necessarily inactivated by the acidic conditions of the stomach, iii) presence of the virus in stool samples and wastewater. This all certainly adds more weight to a faecal-oral route route of transmission for SARS-CoV-2 and the likelihood of COVID-19 being a foodborne disease – don’t you think?
References
An, P., Chen, H., Jiang, X., Su, J., Xiao, Y., Ding, Y., … & Lv, X. (2020). Clinical features of 2019 novel coronavirus pneumonia presented gastrointestinal symptoms but without fever onset. The Lancet. DOI: 10.2139/ssrn.3532530
Gao, Q. Y., Chen, Y. X., & Fang, J. Y. (2020). 2019 novel coronavirus infection and gastrointestinal tract. Journal of Digestive Diseases. DOI: 10.1111/1751-2980.12851
Gu J, Han B, Wang J, (2020). COVID-19: Gastrointestinal manifestations and potential fecal-oral transmission, Gastroenterology. DOI: 10.1053/ j.gastro.2020.02.054.
Guan, W. J., Ni, Z. Y., Hu, Y., Liang, W. H., Ou, C. Q., He, J. X., … & Du, B. (2020). Clinical characteristics of coronavirus disease 2019 in China. New England Journal of Medicine. DOI: 10.1056/NEJMoa2002032
Holshue, M. L., DeBolt, C., Lindquist, S., Lofy, K. H., Wiesman, J., Bruce, H., … & Diaz, G. (2020). First case of 2019 novel coronavirus in the United States. New England Journal of Medicine 382 : 929-936. DOI: 10.1056/NEJMoa2001191
Jin, X., Lian, J. S., Hu, J. H., Gao, J., Zheng, L., Zhang, Y. M., … & Yu, G. D. (2020). Epidemiological, clinical and virological characteristics of 74 cases of coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms. Gut. DOI :10.1136/gutjnl-2020-320926
Lodder, W. & de Roda Husman, A.M. (2020). SARS-CoV-2 in wastewater: potential health risk, but also data source. The Lancet Gastroenterology & Hepatology. DOI: 10.1016/ S2468-1253(20)30087-X
Luo S, Zhang X, Xu H (2020). Don’t overlook digestive symptoms in patients with 2019 novel coronavirus disease (COVID-19), Clinical Gastroenterology and Hepatology (2020), DOI: 10.1016/j.cgh.2020.03.043
